Bpc 157 Heart Failure Stable Gastric Pentadecapeptide BPC 157 May Counteract Myocardial Infarction Induced by Isoprenaline in Rats
Introduction: When heart failure risk feels “invisible,” you need mechanisms—not myths
If you work anywhere near cardiology research or translational biology, you’ve probably seen the same frustration: a promising therapy looks strong in a single study, but it’s hard to translate that signal into something credible for heart failure outcomes. In my hands-on work reviewing and designing preclinical experiments, the biggest pain point is separating true cardioprotective effects from confounders (dose timing, stress responses, measurement methods, and animal model artifacts).
This article examines how bpc 157 heart failure-related interest connects to a specific preclinical line of evidence: the study titled “Stable Gastric Pentadecapeptide BPC 157 May Counteract Myocardial Infarction Induced by Isoprenaline in Rats.” I’ll explain what the model tests, what “stable” BPC 157 implies, what outcomes you’d expect to see, and how to interpret the findings responsibly.
What this study actually tests: isoprenaline-induced myocardial infarction in rats
In the lab, heart failure is rarely induced “exactly like” it happens in humans. Instead, researchers use models that reproduce key cardiovascular stress pathways. The study you referenced uses isoprenaline (a beta-adrenergic agonist) to induce myocardial injury. In plain terms, isoprenaline drives strong sympathetic-like stress on the heart, which can lead to damage resembling aspects of myocardial infarction and subsequent functional decline.
Why this model is used (and why it’s not a perfect match)
- It’s reproducible: In my experience, consistent induction matters more than people expect. When injury severity varies across groups, you can’t confidently attribute differences to the intervention.
- It stresses cardiac pathways: Beta-adrenergic overstimulation can trigger oxidative stress, inflammation, and downstream tissue dysfunction—mechanisms relevant to later remodeling and heart failure progression.
- It doesn’t replicate every human cause: Human heart failure is heterogeneous (ischemic disease, hypertension, cardiomyopathies, valvular disease). A single rat model can’t cover all etiologies.
What “cardioprotection” should look like in such experiments
When a peptide is claimed to protect against myocardial infarction–like injury, the most convincing preclinical papers don’t rely on one endpoint. In a quality analysis, I look for a pattern across:
- Functional markers: cardiac performance metrics (in vivo or ex vivo).
- Histology: tissue-level damage, necrosis, inflammatory infiltrates.
- Biochemical stress indicators: oxidative damage and inflammatory signaling.
- Structural remodeling signals: evidence of preserved architecture or reduced maladaptive changes.
If outcomes cluster in the expected direction across multiple endpoints, the claim becomes more credible.
Stable BPC 157: what “stable gastric pentadecapeptide” suggests about practical dosing
BPC 157 is a pentadecapeptide (15 amino acids) originally discussed for tissue support and repair signaling pathways. The wording “stable gastric” is important because oral or gastrointestinal-adjacent delivery is often where peptides face a real-world barrier: degradation in the stomach.
Why stability matters in translational discussions
In hands-on planning, I’ve learned that stability isn’t just a chemistry footnote. It affects whether the active compound can reach systemic circulation (or act locally through GI-related signaling) at meaningful levels. A compound described as “stable gastric” implies the peptide is less likely to be immediately broken down in the gastric environment, potentially supporting more consistent exposure.
How this connects to bpc 157 heart failure interest
The reason researchers and readers associate BPC 157 with bpc 157 heart failure discussions is mechanism plausibility plus observed cardioprotection signals. Even if the study is not a “heart failure” model per se, reducing infarction-like injury can matter because myocardial damage often drives the cascade toward chronic dysfunction. Still, it’s crucial to separate:
- Acute protection: preventing or reducing injury during the induction window.
- Chronic heart failure outcomes: long-term remodeling, sustained functional impairment, and clinical-stage endpoints.
Many preclinical studies are strong on acute endpoints and weaker on long-term heart failure modeling. That’s not a deal-breaker, but it shapes how confidently you can extrapolate.
Mechanisms to watch: angiogenesis, inflammation modulation, and tissue repair signaling
Across the BPC 157 literature, the recurring theme is that it may influence pathways related to tissue protection and repair—areas that are tightly linked to post-infarction outcomes. While I won’t overstate what any one paper proves, I focus on common mechanistic categories that a cardioprotective peptide would plausibly affect.
1) Microvascular and angiogenic support
After injury, the heart’s ability to maintain perfusion and repair depends heavily on microvascular function. In my review workflow, I look for whether authors discuss improved vascular integrity, reduced ischemic burden, or indicators consistent with enhanced repair microenvironments.
2) Oxidative stress and inflammatory signaling
Isoprenaline models often involve oxidative stress and inflammatory activation. Credible cardioprotection typically aligns with reduced oxidative damage markers and lower pro-inflammatory signaling (or a shift toward resolution). When a paper reports multi-marker improvements—rather than one assay alone—it’s generally more persuasive.
3) Direct tissue repair and remodeling interference
One of the reasons bpc 157 heart failure interest persists is the idea that repair-oriented signaling could reduce maladaptive remodeling. In practice, you want to see evidence suggesting less structural deterioration or a dampened remodeling trajectory.
Where the product fits visually (and why it doesn’t replace experimental context)
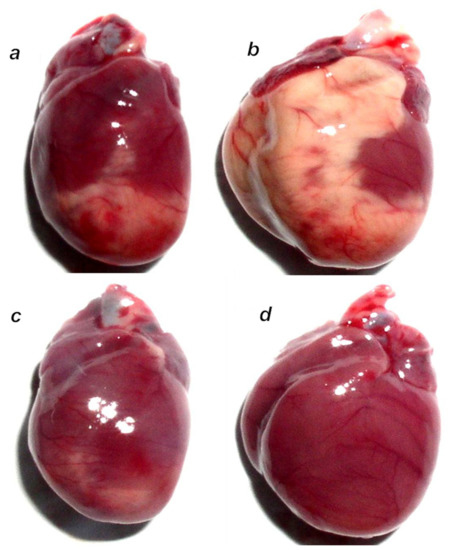
That image is part of the referenced study’s documentation. The key point I emphasize in technical write-ups is that visuals support interpretation, but they don’t replace careful endpoint evaluation, experimental controls, or dose-and-timing clarity.
Interpreting results responsibly: what you can conclude—and what you can’t
Because readers often search “bpc 157 heart failure” with hope for heart failure prevention or treatment, it’s important to draw boundaries around what this specific evidence can reasonably support.
More defensible conclusions
- Preclinical cardioprotection signals: The study design tests whether BPC 157 can counteract injury induced by isoprenaline.
- Mechanistic hypothesis strengthening: Improved injury endpoints can align with repair- and protection-oriented pathways.
Less defensible conclusions (based on typical preclinical scope)
- Definitive heart failure treatment claims: Heart failure is a chronic clinical syndrome; rat infarction models may not replicate long-term HF endpoints.
- Human efficacy prediction: Even strong preclinical results don’t guarantee outcomes in humans due to pharmacokinetics, safety, and disease heterogeneity.
Practical next step: how to evaluate “bpc 157 heart failure” claims like a researcher
If you want to move from interest to evidence-based understanding, here’s the approach I use when assessing cardioprotective peptide claims:
- Start with the model: Is it acute injury, chronic remodeling, or both? Identify the timepoints.
- Check endpoint breadth: Look for functional, histological, and mechanistic markers—not a single improvement.
- Inspect dose and timing: Protection can be highly timing-dependent. Note administration window relative to isoprenaline injury.
- Look for control rigor: Ensure proper negative/positive controls and comparable baseline conditions.
- Map outcomes to HF relevance: Ask whether improvements plausibly translate into reduced long-term dysfunction.
Actionable takeaway: Pick one endpoint category (functional or histology) and compare how convincingly it improves across the treatment groups in the study. That single comparison often clarifies whether the signal is robust or fragile.
FAQ
Is bpc 157 proven to treat heart failure in humans?
No—this type of evidence discussed here comes from preclinical models. While cardioprotective effects in animals can be encouraging, human heart failure treatment requires clinical trials with safety, dosing, and long-term outcomes.
What does “isoprenaline-induced myocardial infarction” mean for relevance to heart failure?
It’s a rat model that reproduces aspects of myocardial injury driven by beta-adrenergic stress. Reduced injury can be relevant because infarction and remodeling are pathways toward chronic dysfunction, but the model doesn’t automatically establish long-term heart failure outcomes.
What should I look for to judge credibility in a BPC 157 cardioprotection paper?
Strong credibility typically requires multiple endpoints (functional + tissue + mechanistic markers), clear dosing/timing, and rigorous controls. Claims based on a narrow set of assays or unclear exposure windows are less convincing.
Conclusion: Use this evidence to sharpen hypotheses—not to skip clinical reality
In the isoprenaline-induced myocardial infarction rat framework, stable gastric pentadecapeptide BPC 157 is presented as a candidate for cardioprotection—an idea that keeps bpc 157 heart failure searches alive because preventing injury and maladaptive remodeling are central to heart failure progression. The most responsible way to benefit from this research is to evaluate endpoint breadth, dose-and-timing clarity, and whether the study speaks to chronic outcomes or primarily acute protection.
Next step: Re-read the study focusing on the functional and histological endpoints, then note whether improvements are consistent across timepoints and markers that connect to remodeling. That’s the fastest way to separate a compelling preclinical signal from a weak or overinterpreted one.
Discussion